
Skip to:
- The Genetics that Underpin Trisomy X
- Manifestations of Trisomy X
- Diagnosing Chromosomal Abnormalities in Females
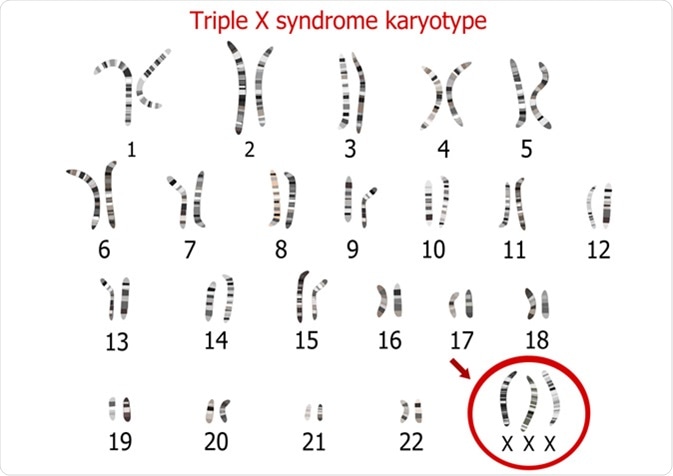
Triple X syndrome, also known as 47, XXX, Triple X, Triplo-X, or trisomy x is a sex chromosome aneuploidy, or chromosome abnormality, in which females have an additional X chromosome. The number and visual appearance of chromosomes in the cell nuclei, known as the karyotype, in trisomy X patients differs from the XX karyotype in typical females.
Typically, females have two XX chromosomes that define sex. in trisomy X, the additional X chromosome brings the total number of chromosomes to 47. This chromosomal abnormality is rare, occurring in approximately 1 in every 1,000 female births.
Other concurring minor conditions displayed by females with trisomy X include congenital heart disease, clinodactyly, and epicanthal folds. Facial dysmorphism, strabismus, genitourinary malformation, and minor hand and feet anomalies, have also been shown to concur with trisomy X.
The Genetics that Underpin Trisomy X
In some cases, the karyotype 47, XXX occurs in a mosaic fashion. Mosaicism refers to the presence of two or more genetically different sets of cells in the body; that is, some cells have 46 chromosomes whereas others have the trisomy X with 47 chromosomes. However, in the majority of cases, the non-mosaic 47, XXX karyotype is present. Mosaicism occurs in approximately 10%, with 46, XX/47, XXX or 47, XXX/48, XXXX. Others may have another genetic abnormality called Turner syndrome in which females have one of their X chromosomes either partly or completely missing.
The origin of trisomy X syndrome is what is known as maternal nondisjunction errors during meiosis. This is the failure of homologous chromosomes (chromosomal pairs) to separate properly after cell division, which leads to chromosomal imbalance or aneuploidy. At present only 10% of individuals with trisomy X are diagnosed; despite the high incidence compared to many genetic disorders. This is because of the subtle and nonspecific manifestations of the condition – as such they do not prompt genetic testing.
Manifestations of Trisomy X
Females with this chromosomal abnormality demonstrate variability in their phenotype, which includes physical and psychological features. Some females demonstrate mild symptoms, whereas others have significant features. The majority of females born with trisomy X show no symptoms at birth. Their height tends to vary as they grow, ranging from short statures to higher than average in most cases; in addition, IQ tends to be lower than average but there are no specific atypical behavioural patterns observed. In cases where developmental and behavioral conditions present, there may be delays in speech and motor skills, attention-deficit/hyperactivity disorder (ADHA), anxiety, and other mood disorders present.
The most common physical features include hypertonia, clinodactyly, tall stature, developmental delays, learning, and intellectual disabilities, ADHD, psychiatric conditions including anxiety and mood disorders, renal and genitourinary abnormalities and premature ovarian failure. The symptoms correlate with the most strongly affected brain regions which are associated with learning and motor control.
Diagnosing Chromosomal Abnormalities in Females
The diagnosis of triple X syndrome is made through a process called cytogenetic karyotype testing or microarray analysis. Cytogenetic karyotype testing is an examination of chromosomes that identifies the chromosomal number and any abnormalities. Microarrays enable duplications of entire chromosomes to be detected. Prenatal diagnosis, by contrast, is made by amniocentesis or chorionic villi sampling. Patients diagnosed in the prenatal period tend to have better outcomes as early intervention therapies are implemented when needed.
Owing to a high number of cases not presenting any physical abnormalities, the majority of females with the condition do not seek medical attention nor have their chromosomes tested. The condition often remains undiagnosed until adulthood, when the chromosomal abnormality is detected for reasons of primary amenorrhea. Patients you do present with symptoms are diagnosed earlier in childhood.
Early studies have suggested that the diagnosis of Triple X syndrome leads to better outcomes in females with respect to neurodevelopmental outcomes, including IQ and decreased the frequency of academic difficulties and psychiatric conditions. However, these studies were limited by their small sample size and design. More comprehensive studies took a longitudinal approach whereby the females who were identified prospectively were monitored as part of a multi‐centre study of sex chromosome aneuploidies.
These studies highlighted that intellectual disabilities seen in triple X syndrome patients fell within the normal range, although mean IQ points were 10-15 points lower than their sibling controls. They were also identified as high-risk for the development of learning and development programme, psychological difficulties and motor deficits. In a more recent study which analysed 74 females, the outcomes echoed earlier studies; finding that prenatally diagnosed females fare better with regards to cognitive and functional outcomes. However, these females are still at risk for neurodevelopmental disorders. As a result, genetic counselling is recommended.
Sources
- Otter, M. et al. Triple X syndrome: a review of the literature. Eur J Hum Genet. (2010) doi: 10.1038/ejhg.2009.109
- Bender, B.G. et al. Neuropsychological and functional cognitive skills of 35 unselected adults with sex chromosome abnormalities. Am J Med Genet. (2001) doi: 10.1002/ajmg.1490
- Grosso, S. et al. Electroencephalographic and epileptic patterns in X chromosome anomalies. J Clin Neurophysiol. (2004) doi: 10.1097/00004691-200407000-00003
- Robinson, A., Bender, B., Borelli, J. et al. Sex chromosomal anomalies: Prospective studies in children. Behav Genet 13, 321–329 (1983). https://doi.org/10.1007/BF01065770
- Linden, M.G. et al. Bender BG. Fifty-one prenatally diagnosed children and adolescents with sex chromosome abnormalities. Am J Med Genet. (2002) doi: 10.1002/ajmg.10394
Further Reading
- All Triple X Syndrome Content
Last Updated: Feb 6, 2020

Written by
Hidaya Aliouche
Hidaya is a science communications enthusiast who has recently graduated and is embarking on a career in the science and medical copywriting. She has a B.Sc. in Biochemistry from The University of Manchester. She is passionate about writing and is particularly interested in microbiology, immunology, and biochemistry.
Source: Read Full Article